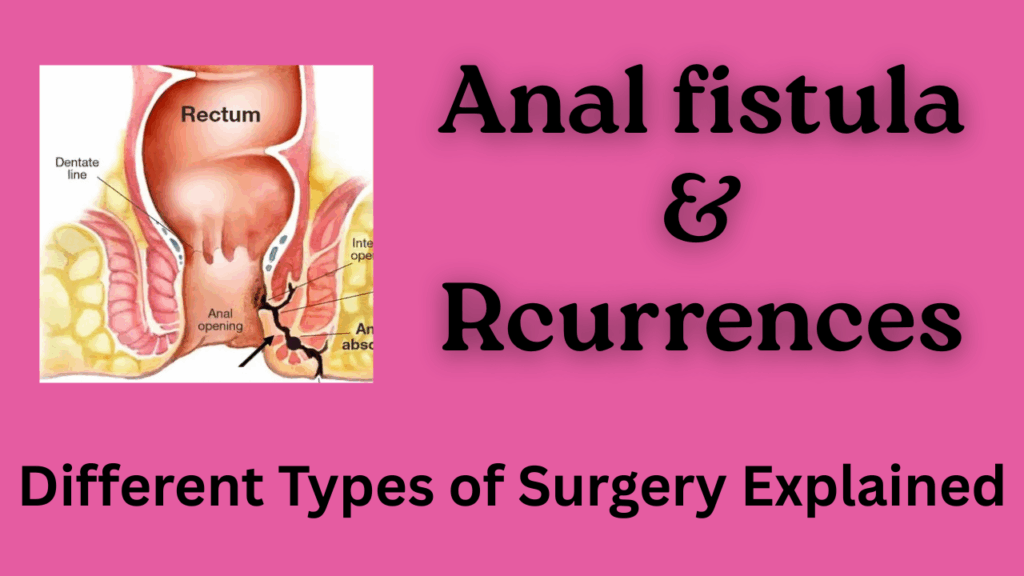
An anal fistula is an abnormal tunnel that connects the inside of the anal canal or rectum to the skin around the anus. It usually follows an infected anal gland or abscess and causes pain, discharge, intermittent swelling, and sometimes repeated infections. Treatment is primarily surgical because simple measures rarely cure the tract; choice of procedure depends on fistula anatomy (low vs high, simple vs complex), sphincter involvement and patient factors. PubMed Central+1
1. Fistulotomy in Anal Fistula
What it is: The fistula tract is laid open (opened along its length) so it heals from the base upward. It is the common operation for simple, low fistulas.
Recurrence / outcomes: For simple low fistulas fistulotomy gives very high healing rates. Many series report healing >90% with low recurrence (single-study recurrence figures often under 10%). But for high or complex fistulas, recurrence is higher, depending on complexity. Studies quote low-fistula recurrence around 6% and higher-fistula recurrence up to ~28% in some cohorts. Fistulotomy has a higher risk of incontinence when used for fistulas that cross significant sphincter muscle, so patient selection is key. ScienceDirect+2Nature+2
2. Fistulectomy in anal fistula surgery.
What it is: The entire tract and surrounding tissue are excised (cut out) rather than simply opened.
Recurrence / outcomes: Healing rates are generally good for selected cases; some series show similar healing to fistulotomy but with somewhat higher wound complications and potentially higher incontinence risk if much the External sphincter muscle is removed. Comparative series report recurrence figures roughly comparable to fistulotomy (single-study examples showed recurrence around 9–12% at short follow-up), but results vary with fistula complexity and technique. Journal of Population Therapeutics+1
3. Core excision (coring-out of anal fistula tract)
What it is: The tract is “cored out” leaving surrounding sphincter muscle intact, aims to remove infected tissue while sparing external sphincter muscle.
Recurrence / outcomes: Recent series report good healing and modest recurrence: one multicentre study reported healing ~92% and recurrence 8.8% among healed patients (treatment success ~84%). This technique can be a good sphincter-sparing option for selected fistulas. PubMed Central
4. LIFT procedure (ligation of intersphincteric fistula tract)
What it is: The fistula tract is approached in the intersphincteric plane, the tract is ligated/ divided and the internal opening is closed. Remaining distal tract is excised. This is a sphincter-sparing technique intended for trans-sphincteric fistulas.
Recurrence / outcomes: Meta-analyses and systematic reviews report variable results. Pooled analyses commonly show success around 70–80% (so recurrence roughly 20–30% in many series), though some original LIFT reports showed recurrence as low as ~9–10% and modified techniques may give different results. Predictors of failure include horseshoe fistulas, Crohn’s disease and previous surgery. LIFT is attractive because it preserves continence in most patients. PubMed+2ResearchGate+2
5. Seton placement (cutting seton / draining seton / staged procedures)
What it is: A thread or rubber band (seton) is placed through the tract. It is similar to ksharsutra in Ayurved, but a different type of thread is used. A draining seton keeps the tract open to drain until definitive surgery, while a cutting seton gradually divides the sphincter with fibrosis to allow healing. Setons are often used for complex or high fistulas, or before definitive sphincter-sparing repair.
Recurrence / outcomes: Outcomes vary by seton type and technique. Cutting setons reports high primary “success” in many series (some report 80–100%), but there are concerns about incontinence. Pulling/seton techniques in comparative reports have shown recurrence rates in the teens (for example, 13–14% in some series), while other studies report wider ranges. Many surgeons use setons as part of a staged strategy rather than as the single definitive step. PubMed Central+1
6. VAAFT (video-assisted anal fistula treatment)
What it is: It is an Endoscopic (video) inspection of the tract with internal cleaning/fulguration and closure of the internal opening. Minimally invasive and sphincter-sparing surgery. It requires a special type of fistula scope and laparoscopy setup.
Recurrence/outcomes: Published series show variable recurrence: some series report recurrence rates around 15–30%, with higher recurrence in previously operated/recurrent fistulas. VAAFT is promising for selected patients, but long-term comparative data are still evolving. LWW Journals+1
7. Ksharsutra procedure (medicated seton ,traditional Ayurvedic technique)
What it is: A medicated thread (ksharasutra) is passed through the tract and changed periodically; it promotes gradual cutting, chemical debridement and healing. It remains commonly used in the Indian subcontinent. This is specially done by ayurved surgeons.
Recurrence / outcomes: Several trials and series report moderate recurrence in experienced hands. Long-term series with recurrence rates reported as low as 15 to 20 % at multi-year follow-up. Reported success depends on technique, follow-up duration and operator experience. Comparative randomised data are limited, but ksharsutra remains an accepted option where available and when performed by experienced practitioners. PubMed Central+1
What the literature says about overall recurrence after anal fistula surgery
Systematic reviews and pooled analyses show substantial heterogeneity: reported recurrence rates after anal fistula surgery across procedures and studies range widely (commonly quoted pooled recurrence ~15–20% but individual study ranges from ~3% up to >40% depending on procedure mix, fistula complexity and follow-up). Key predictors of recurrence are failure to identify/close the internal opening, complex fistula anatomy (high/trans-sphincteric/horseshoe), Crohn’s disease, prior surgery and inadequate drainage or infection control. ScienceDirect+1
Final opinion (practical takeaways) for anal fistula management
- Tailor the operation to the fistula type. For simple, low fistulas a fistulotomy often gives the best chance of cure with low recurrence. For high or complex fistulas choose a sphincter-sparing approach (LIFT, core excision, VAAFT, staged seton ± flap) to reduce incontinence risk even if recurrence risk is modestly higher. ScienceDirect+1
- Expect variability. No single technique guarantees the eradication of all fistulas. Recurrence rates vary by complexity, prior surgery and surgeon experience. Discuss the trade-off clearly with the patient: cure probability vs continence risk. ScienceDirect
- Operator experience matters. Techniques like ksharsutra, VAAFT and modified LIFT show best results in centers and hands familiar with the procedure, results in the literature vary accordingly. PubMed Central+1
- Identify and manage the internal opening. Failure to identify/close the internal opening is a leading cause of recurrence. Careful preoperative assessment (MRI/endoanal ultrasound when needed) and intraoperative strategy reduce recurrence. PubMed Central

FAQ
Which surgery has the lowest recurrence for anal fistula?
For simple low fistulas, fistulotomy often has the lowest recurrence and fastest cure rates. For complex/high fistulas, sphincter-sparing options (LIFT, core excision, staged seton strategies) aim to balance cure with continence; recurrence rates vary, and no single method is universally best.
Can recurrence be predicted or prevented?
Yes, known risk factors include complex anatomy, Crohn’s disease, prior failed operations and failure to locate/close the internal opening. Using imaging (MRI) for complex cases and choosing an appropriate sphincter-sparing technique reduces recurrence risk.
What happens if a fistula recurs?
Recurrent fistulas often require re-evaluation (imaging), and treatment is individualised. Options include repeat sphincter-sparing procedures, seton placement, advancement flaps, VAAFT, or sometimes staged approaches. Multiple surgeries may be required in recurrent disease.
Is non-surgical treatment effective?
Non-surgical measures (antibiotics, sitz baths) can control symptoms and infection, but generally don’t cure established fistula tracts. Minimally invasive adjuncts (fibrin glue, plugs) have variable success and higher recurrence rates compared with definitive surgical procedures.
How important is surgeon experience and follow-up?
Very important , outcomes (recurrence and continence preservation) correlate strongly with surgeon experience, correct technique selection and adequate follow-up to detect and treat early failure. Discuss expected follow-up schedule and red flags (new discharge, pain, fever) at the time of consent.


